
HPV and its Link to Cervical Cancer
Dhwani Patel, Ching Yung Yuan, Mackenzie Smith
January 2024
1 in 168 women is expected to develop cervical cancer during her lifetime (1). Cervical cancer affects the cervix of a female, which is the canal connecting the uterus to the vagina. Cervical cancer can lead to heavy bleeding, fertility issues and death (1). There are many risk factors associated with cervical cancer including environment, genetics, and lifestyle choices such as smoking (1). However, the most common and the most serious risk factor for cervical cancer is infection with Human papillomavirus (HPV) (1). According to the World Health Organization, untreated HPV infection causes 95% of cervical cancers (2).
HPV Infection and Transmission
HPV infects the mucous-producing surfaces of the body, such as the lining of the genital tract and the inside of the oral cavity (3). For the infection to take place, the HPV virus must first breach the surface tissue layer at these sites (3). Usually, this occurs when the HPV virus enters the surface tissue via pre-existing lesions or mechanical damage (e.g. cuts and other wounds) (3). However, on occasion, inflammation can also compromise the tissue’s surface layer and create an opportunity for HPV to enter the tissue (3). Once an infection has occurred, the HPV virus hijacks human host cells and turns them into virus-producing factories (3). This damages the cell and leads to more viral particles that invade neighbouring cells until the infection takes over large swaths of mucosal surface tissue (Fig. 1) (4).
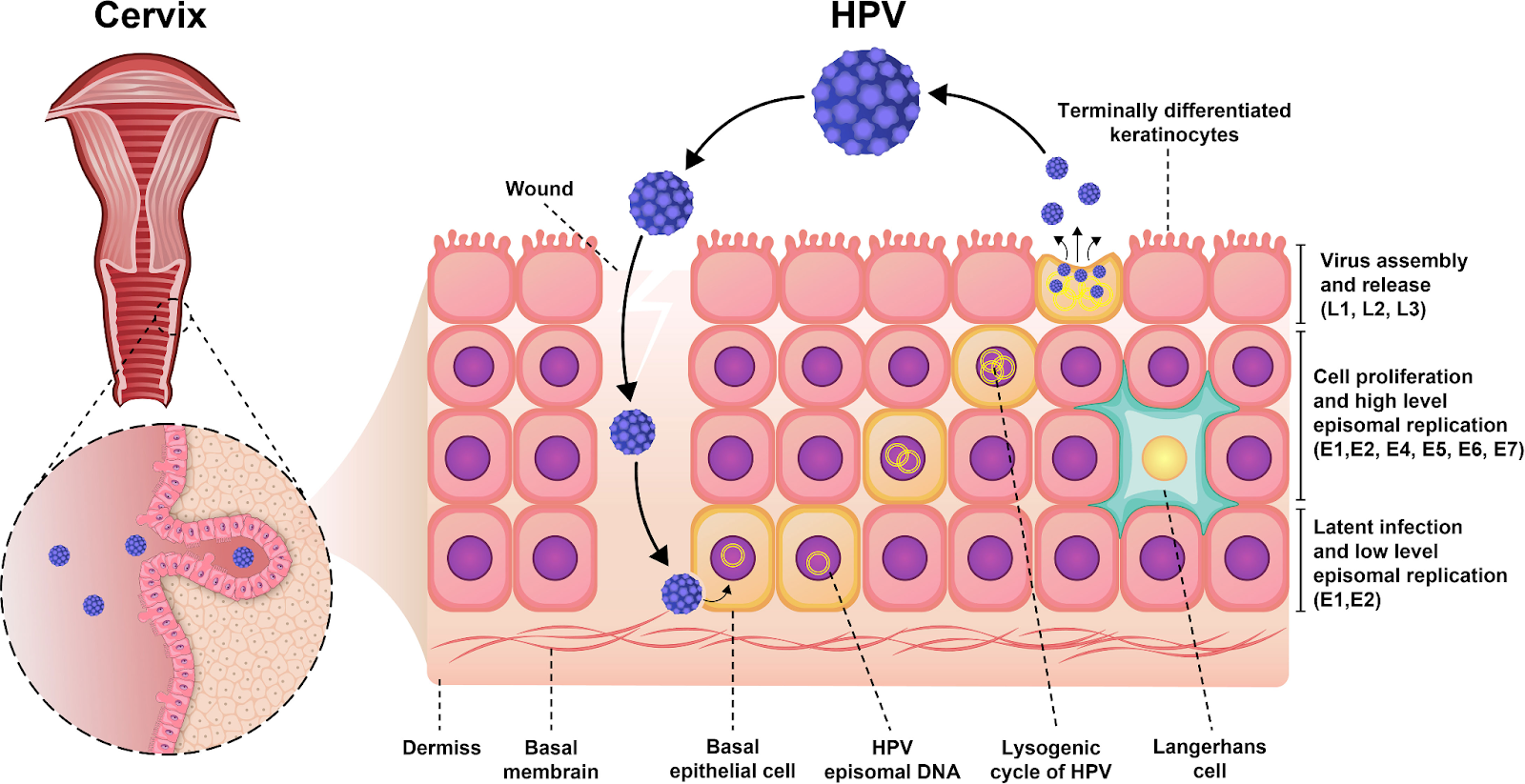
Figure 1. HPV infection of surface tissue at the cervix (4). HPV bypasses the protective surface layers at the cervix by entering the tissue through a lesion. The viral life cycle, from infection to the production of more HPV viruses, is shown within the image.
There is no test for an individual’s HPV status (5). Quite often the infected individual is unaware of having HPV since most infected individuals do not show any symptoms (e.g. warts at the oral or genital site of infection) (5). Individuals with or without symptoms are both capable of spreading the virus (5). HPV is transmitted through skin-to-skin contact or skin-to-mucosa contact (6). This includes sexual activity with an infected individual, or through non-sexual contact, such as coming in contact with contaminated objects or an infected individual with poor hand hygiene (6). Vertical transmission, an infection transmitted from the infected mother to the newborn through contact with infected amniotic fluid, placenta, or genital mucosa during birth, is also a possible method of acquiring the virus (6).
In most cases (90% of the time) the body’s immune defence mechanisms can eliminate the virus within two years (5). However, if the HPV virus persists at the site of infection, this can lead to persistent, periodic flare-ups of genital warts or contribute to an increased risk of cancer at the site of infection (5).
HPV as a Risk Factor for Cervical Cancer
The risks of cervical cancer are greatly increased with repeated HPV infections (7). Not all HPV strains lead to cancer, however, the HPV virus can alter the host cell’s DNA machinery, which over decades can cause that host cell to turn cancerous (7).
There are more than 170 strains of HPV, only the high-risk strains are known to cause cervical cancer (8). On the other hand, low-risk variants of HPV (e.g. HPV 6, HPV11) are associated with genital warts (9). There are twelve high-risk HPV strains in total, in particular, HPV 16 and HPV 18 are especially prominent as they cause up to 70% of all cervical cancers (8).
HPV Vaccination
The best method to prevent HPV-related cervical cancer is via vaccination, which is almost 100% effective at preventing HPV infection (10). There are currently 3 vaccines on the market which all offer protection against HPV infections and genital warts caused by HPV (10). All 3 types of vaccines are made from empty viral capsids (the ‘shell’ of the virus made of viral proteins) (10). Because the vaccines only contain the outer shell of the virus, the vaccines do not contain any infectious material capable of causing the symptoms of HPV infection (10). This makes the HPV vaccines very safe to administer broadly across different populations – even individuals who are immunocompromised can take the vaccine (10). When the vaccines are injected into the body, our immune cells learn to recognize these virus shells so that, in case of a real HPV infection, the vaccine-induced recognition system can immediately kick in and rid the body of HPV (10). In the absence of vaccination, the body’s immune cells must first learn to recognize the HPV virus and then get rid of the virus, all while the infection is ongoing (10). Vaccination shortened the ‘immune learning’ process significantly to give infected individuals a better fighting chance against HPV infections (10).
Cervarix
Cervarix protects against two strains of HPV (HPV 16 and HPV 18) (11). Cervarix has been in circulation since 2010, therefore there is already a decade of data approving of its usage and safety (11). Cervarix is recommended for women and girls from the age of 9-45 ages (11). The vaccination requires 3 doses over 6 months via intramuscular injection, which may lead to soreness at the sight of the injection (11). Other side effects include headache, fatigue, and joint and muscle pain, as well as gastrointestinal symptoms (11).
Gardasil and Gardasil9
Gardasil protects against 2 high-risk strains of HPV (HPV 16 and HPV 18) as well as 2 prominent low-risk strains of HPV (HPV 6 and HPV 11) which in total cause 90% of all HPV-related genital warts (12). Gardasil9 protects against the same 4 strains as Gardasil but also protects against 5 additional high-risk strains of HPV. Gardasil was first introduced in 2006 whereas Gardasil9 came later, in 2014 (12,13). Nevertheless, these two vaccines have been used for over a decade with great benefits (12,13). Gardasil and Gardasil9 are approved for usage by all individuals, male and female, between 9-45 years of age (12,13). The extended recommendation for boys and men is due to the effectiveness of HPV vaccination against HPV-related oropharyngeal cancer, anal cancer, and penile cancer which in recent years have seen rising incidence among the male population (13). Gardasil and Gardasil9 are both taken in 3 separate doses over 6 months (12,13). The intramuscular injection method may lead to muscle soreness at the injection. Additionally, Gardasil and Gardasil9 have been known to cause fainting (12,13).
Screening for HPV
Fortunately, screening protocols for cervical cancers have become standardized in Canada. If you are a sexually active female who is 21 years of age or older, it is recommended that you have a Pap test repeated every 3 years to detect abnormal cells before they fully transform into cancer (14). In addition, HPV testing can be used in combination with the Pap test (14). It is important that women continue to be regularly screened for cervical cancer even after vaccination, as the vaccine protects against most, but not all HPV types (14). For more information on cervical cancer screening please visit the Canadian Cancer Society website.
References
1. Harnessing the potential of CAR-T cell therapy: progress, challenges, and future directions in hematological and solid tumor treatments | Journal of Translational Medicine | Full Text. https://translational-medicine.biomedcentral.com/articles/10.1186/s12967-023-04292-3.
2. Guzman G, Reed MR, Bielamowicz K, Koss B, Rodriguez A. CAR-T Therapies in Solid Tumors: Opportunities and Challenges. Current Oncology Reports. 2023;25(5): 479–489. https://doi.org/10.1007/s11912-023-01380-x.
3. Roschewski M, Longo DL, Wilson WH. Chimeric Antigen Receptor T-cell Therapy for Large B-cell Lymphoma: Who, When, and How? The New England journal of medicine. 2022;386(7): 692–696. https://doi.org/10.1056/NEJMe2118899.
4. Advantages of CAR-T Cell Therapy | Rutgers Cancer Institute of New Jersey. https://www.cinj.org/patient-care/advantages-car-t-cell-therapy.
5. Han D, Xu Z, Zhuang Y, Ye Z, Qian Q. Current Progress in CAR-T Cell Therapy for Hematological Malignancies. Journal of Cancer. 2021;12(2): 326–334. https://doi.org/10.7150/jca.48976.
6. Adkins S. CAR T-Cell Therapy: Adverse Events and Management. Journal of the Advanced Practitioner in Oncology. 2019;10(Suppl 3): 21–28. https://doi.org/10.6004/jadpro.2019.10.4.11.7. CAR T Cells: Engineering Immune Cells to Treat Cancer – NCI. https://www.cancer.gov/about-cancer/treatment/research/car-t-cells.
